What are orofacial clefts (OFCs)?
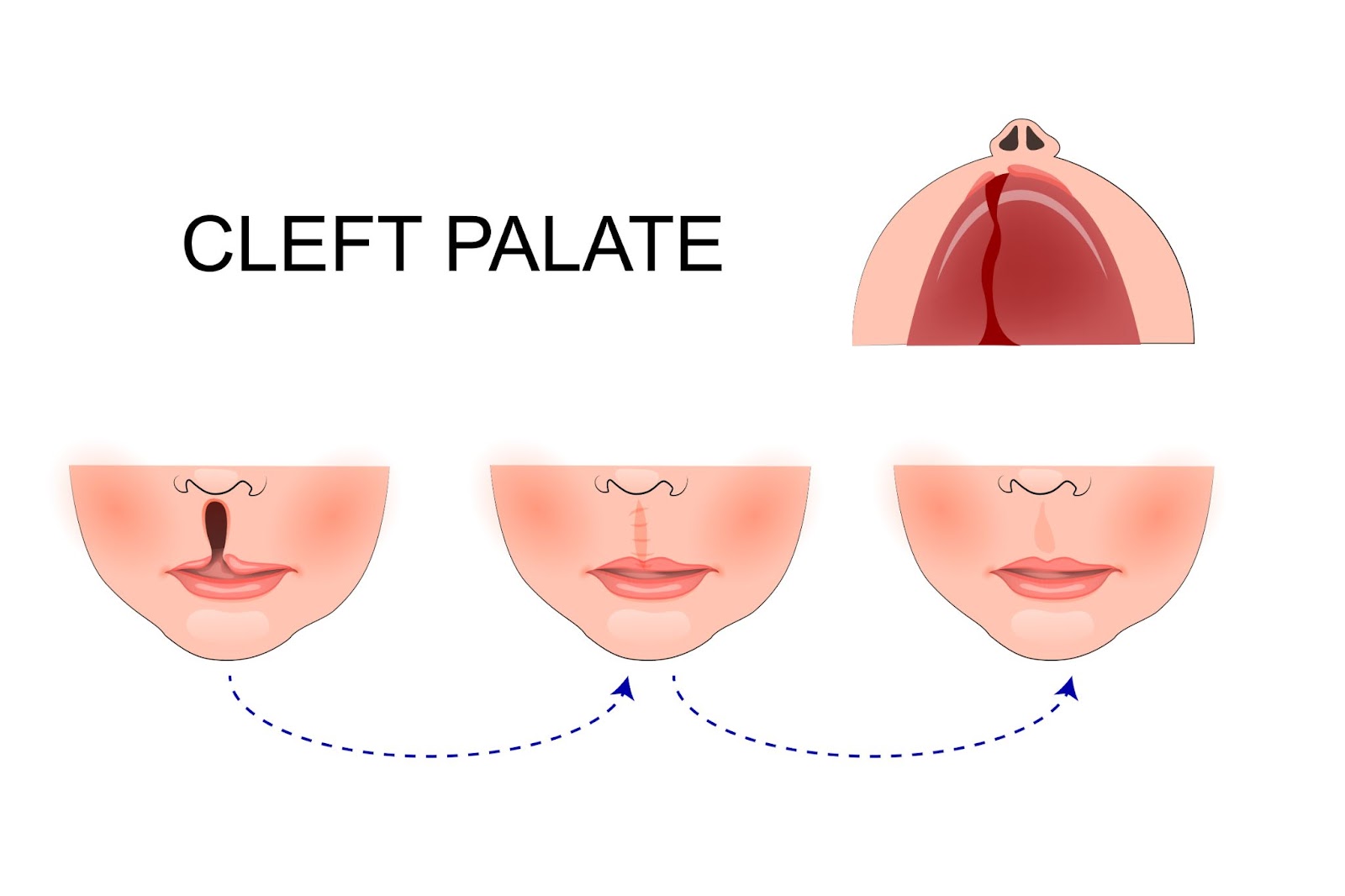
Orofacial clefts (OFCs) are a group of birth anomalies which occur during fetal development, and refer to cleft lips, palates (the roof of the mouth), or a combination of both. When in the womb, the lip and mouth both form during the first trimester (CDC).
Depending on the individual, both types of OFCs can range in severity. A cleft palate can extend all the way to the nose, contributing to a wide variety of health issues that impacts an individual’s ability to eat, speak, and more (Mayo Clinic). A cleft lip can extend all the way to the nasal cavity, and can be on one side of the mouth or on both.
It is not uncommon to see poverty compound the health effects caused by OFCs. Middle African countries contain the highest rates of cleft-related malnutrition. In countries such as Ethiopia—where Alliance for Smiles is headed to this summer, in 2023—food insecurity is more widespread than any other country in the world. As a result, individuals with OFCs are some of the most vulnerable populations to face death due to starvation, infection, and other related factors (IHME).
Another recent study, conducted by the Children’s Hospital of Philadelphia (CHOP), looked at over six million births in the U.S. to review the links between poverty and developing cleft lip/palate. The findings concluded that the mother’s physical health is directly linked to the birth defects.
The CHOP study stratified data by maternal income, health conditions, access to health care, and other key indicators of living in poverty. The results showed that lower socioeconomic classes possess higher rates of children with OFCs compared to higher socioeconomic groups.
Additionally, the researchers found that stigma associated with OFCs lead to social discrimination and impacts an individual’s chance of employment. Living in poverty not only exacerbates the health effects caused by these conditions, but further imbeds the person’s existence into a lower socioeconomic class, ingraining the individual in a vicious cycle of poverty.
What causes cleft lips and palates to form?
 A number of contributors lead to OFCs emerging in a fetus. The mother’s preexisting physical conditions can place the baby at a higher risk, including a various range of genetic disorders, chronic illnesses, and body weight, whether the mother is obese or underweight.
A number of contributors lead to OFCs emerging in a fetus. The mother’s preexisting physical conditions can place the baby at a higher risk, including a various range of genetic disorders, chronic illnesses, and body weight, whether the mother is obese or underweight.
Alongside this, the mother’s exposure to harmful substances during pregnancy heightens risk. Smoking, drinking alcohol, and substance abuse directly correlate with OFCs appearing in the fetus (Mayo Clinic). Research shows that certain prescription drugs may also heighten risk, such as anti-seizure medication (CDC), as well as environmental factors, such as high pollution (Children’s Hospital Los Angeles).
What health concerns are caused by OFCs?
As a direct cause of the lip and/or mouth’s incomplete formation, an individual with a cleft lip and/or palate may experience difficulties eating and drinking. Food and liquids are prone to escape through gaps in the mouth, and as a result, can lead to malnourishment, growth stunting, and in extreme cases, hunger-related death (IHME).
 According to the IHME, children with a cleft lip and/or palate are twice as likely to be malnourished compared to the global population. Food insecurity can exacerbate the health risks posed by having a cleft lip/palate.
According to the IHME, children with a cleft lip and/or palate are twice as likely to be malnourished compared to the global population. Food insecurity can exacerbate the health risks posed by having a cleft lip/palate.
On top of this, OFCs cause a higher risk of developing pneumonia because of food and liquid entering the lungs through the nasal cavity (IHME). Since the nose and sinuses’ formation may be abnormal, the individual’s hearing is often impacted, and they are more likely to acquire ear infections (Mayo Health). In the mouth, OFCs can impair tooth development, speech, and language development (CDC).
Alongside health concerns, a range of social and emotional impacts are caused by OFCs. Individuals may encounter social exclusion and prejudice, which directly ties in with lowered self-confidence and higher rates of mental disorders. As a result, it is vital for OFCs research to take on a holistic approach in order to understand ways to fully support communities with OFCs, especially in countries where the rates of cleft lips and palates are highest.
What is the prevalence of OFCs in developing countries? How are OFCs linked to poverty?
A systematic review performed by the University of Hong Kong in 2018 revealed that Chinese and other Asian groups experience the highest prevalence of cleft lips and palates, in comparison to other racial groups.
 In China, the Southwest provinces experience the highest rates. Guizhou—a large province in Southwest China—sees 2.08 children born with a cleft lip and/or palate for every 1,000 children born. Because of this, in earlier years, much of Alliance for Smiles’ work was focused on Chinese provinces, such as Guizhou. In these areas, we helped to build the expertise needed to manage these cases locally and sustainably.
In China, the Southwest provinces experience the highest rates. Guizhou—a large province in Southwest China—sees 2.08 children born with a cleft lip and/or palate for every 1,000 children born. Because of this, in earlier years, much of Alliance for Smiles’ work was focused on Chinese provinces, such as Guizhou. In these areas, we helped to build the expertise needed to manage these cases locally and sustainably.
It is not uncommon to see poverty compound the health effects caused by OFCs. Middle African countries contain the highest rates of cleft-related malnutrition. In countries such as Ethiopia—where Alliance for Smiles is headed to this summer, in 2023—food insecurity is more widespread than any other country in the world. As a result, individuals with OFCs are some of the most vulnerable populations to face death due to starvation, infection, and other related factors (IHME).
Another recent study, conducted by the Children’s Hospital of Philadelphia (CHOP), looked at over six million births in the U.S. to review the links between poverty and developing cleft lip/palate. The findings concluded that the mother’s physical health is directly linked to the birth defects.
The CHOP study stratified data by maternal income, health conditions, access to health care, and other key indicators of living in poverty. The results showed that lower socioeconomic classes possess higher rates of children with OFCs compared to higher socioeconomic groups.
Additionally, the researchers found that stigma associated with OFCs lead to social discrimination and impacts an individual’s chance of employment. Living in poverty not only exacerbates the health effects caused by these conditions, but further imbeds the person’s existence into a lower socioeconomic class, ingraining the individual in a vicious cycle of poverty.
What are treatments of/for cleft lips and palates?
It is recommended for children to receive cleft repair surgery between the ages of one to two, if possible. Without early intervention, individuals who receive the surgery later in life may need to receive continuous special dental care, speech therapy, and other accommodations (Mayo Clinic).
Outside of clinical assistance, social support groups help to provide safe, inclusive spaces and ensure individuals with OFCs do not feel isolated from their community. All members of any community should continue to work against preexisting stigma and prejudice that they hold. A physical feature does not strip anyone of their value and significance.
At Alliance for Smiles, we send medical teams to various hospitals and clinics throughout Central and South America, Asia, and Africa to offer free cleft surgeries to underserved, remote communities. Currently, our team is preparing to travel to Ethiopia in May and Vietnam in June —donate here to help fund surgeries in these upcoming locations and the training and equipment needed to help local medical teams serve children with cleft conditions on their own.

